
Pedagogical Approach with Body Interact | Curricular Integration in Healthcare-based Curriculum
What is curricular integration?
Curricular integration is the deliberate design and coordination of learning objectives, content, teaching methods, and strategies, and assessment across disciplines and over time so that students can connect basic, clinical, and professional knowledge and apply it coherently to real patient care. This process avoids implementing learning activities as isolated add-ons embedded in the curriculum.
In medical and nursing education, curricular integration means asking not only whether students will use a Virtual Patient, but also why, when, how, and with what educational purpose. A Body Interact virtual patient should be linked to the appropriate student level, curriculum stage, and teaching approach. This is especially important in healthcare curricula, where learning activities need to contribute to clinical reasoning, communication, patient safety, and readiness for practice.

Key Aspects of Curricular Integration
A strong curricular integration strategy usually includes five core elements.
-
Alignment with learning objectives, outcomes, and competencies
Each Virtual Patient should be mapped to specific competencies, learning objectives, and outcomes of the curriculum.
-
Thoughtful placement in the learner journey
Virtual Patients should be positioned at a suitable stage of training. Early learners (preclinical years) may need guided cases focused on history-taking, data gathering, and physical examination assessment or introduction to clinical reasoning, while advanced learners (clinical years) may benefit from more complex situations where prioritization and time pressure are part of the learning experience.
-
Integration with teaching and assessment
Curricular integration is more powerful when Virtual Patients are embedded into existing pedagogical strategies of the curriculum, such as Problem-Based Learning, Flipped Classroom, Team-Based Learning, etc., and linked to prior knowledge, pre-class preparation, debriefing, reflective tasks, and assessment.
-
Faculty facilitation
Integration depends on faculty adoption and comprehension of, not only how the software and cases work, but also where and why they make sense in the clinical curriculum, to have time to prepare classes and contents so that cases are used consistently across the curriculum. So, ensuring that the professor’s journey is smooth is also essential.
-
Continuous quality improvement
Integrated use should be reviewed over time through learner feedback, analytics, attempts, decisions, timing, and outcomes.
Benefits of integrating Body Interact Virtual Patients into the curriculum
Promotes continuous clinical exposure
With Virtual Patients, the opportunities for realistic clinical exposure and training are no longer dependent on the existence of patients with the pathologies and clinical presentations the curriculum aims.
Strengthens clinical reasoning and decision-making
Body Interact’s design around evolving cases, decisions, timing, and outcomes makes it well-suited for reasoning-focused learning rather than a passive approach.
Provides a safe environment for practice
Students can make mistakes, test hypotheses, and learn from consequences without risk to real patients.
Support flexible and repeated practice
Access to Body Interact scenarios can be done synchronously and asynchronously, with repeated attempts, and receive automated feedback, which supports self-directed learning and deliberate practice.
Standardizes clinical exposure across learners
Integrated Virtual Patients into the curriculum ensures that all learners encounter core clinical presentations, priority conditions, and are exposed to the required competencies, even when real-world clinical exposure is uncertain.
Supports multiple curricular models
Body Interact can be used for synchronous teaching, asynchronous assignments, remediation, merged with a flipped classroom, or other pedagogical approaches and activities, and assessment, it is adaptable across different course designs and levels – from pre to postgraduate.
Generates actionable data for educators
Trackable progress and analytics, which can help instructors identify learner gaps, monitor progression, and refine teaching, are collected in the Bdy Interact Learning Management System.
Best Practices for Curricular Integration
To integrate Body Interact effectively into a medical or nursing curriculum, the following practices are especially valuable:
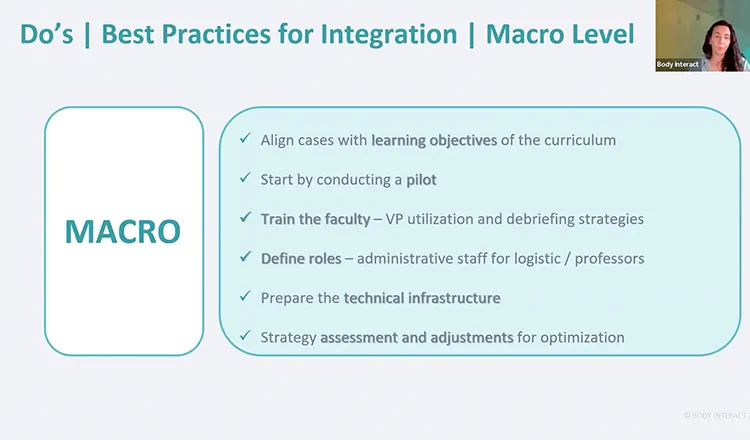
Case Alignment
- Align cases with the learning objectives of the intended outcomes and curriculum objectives.
- Avoid using cases only because they are interesting. Select them because they address required competencies, presentations, or professional tasks.
Faculty Preparation
- A good Virtual Patient case does not guarantee a good learning experience. Faculty need preparation in: how to use the software, how to frame the case, guide discussion, use analytics from the Learning Management System, and connect performance to evidence and standards.
- Successful implementation requires educators to understand the core concepts of simulation-based education (prebriefing, briefing, feedback, and debriefing).
Roles Definition
Faculty frequently report time constraints, so defining roles (administrative staff – logistics / professors – teaching and assessment, etc.), providing protected time, and recognition in successful integration may be helpful in this process.
Teaching Strategy
A defined learning cycle and teaching strategy should be defined, either the same across the curriculum, or defined per signature, module, or course.
Scaffold Complexity Over Time
Either at a macro (overall curriculum) or micro (signature or course) level, it is suggested to begin with guided cases and gradually increase ambiguity and independence, as learners advance.
Integrate into existing Pedagogical Approaches
- Virtual Patients can be successfully integrated into existing pedagogical and methodological approaches of the curriculum, from Problem-Based Learning to Flipped Classroom.
- Take into consideration when integrating Virtual Patients, the size of the group of students (individual > small> medium> large), the context in which it will be used (classroom> simulation center > home), the format in which it will be delivered (Online > In-Person > Blended) and the learning stage of students (Acquisition > Integration > Assessment of knowledge, skills and attitudes).
Debrief
Literature on simulation-based learning reflects on the importance and relevance of debriefing – debriefing transforms experiences into learning.
Student Orientation
Promote student orientation and engagement. Use a low-stakes onboarding case and explicit success criteria in each case (e.g., hypothesis generation, prioritized differential, safe initial management).
Technical Infrastructure
Inadequate infrastructure, device variability, connectivity issues, and lack of support undermine trust and participation. So, do a minimum technical readiness checklist (devices, bandwidth, logins, LMS integration, support contacts internally with the IT team, and externally directly to our support team) and provide a rapid help pathway during sessions.
Review Implementation
Use learner feedback, performance data, and case analytics to improve case selection, timing, difficulty, and assessment alignment.

Explore the rich testimonial on this matter by Prof. Jessy Escobar, from UNITEC and UVM, Mexico.
Curricular integration is what transforms a Virtual Patient from a useful digital activity into a meaningful component of healthcare education. When Body Interact is aligned with outcomes, embedded in sound pedagogical approaches, supported by debriefing, and reviewed to optimize the use of Virtual Patients, it can strengthen clinical reasoning, standardize learning opportunities, and enrich medical and nursing curricula across face-to-face, hybrid, and distance-learning formats.
Explore more: Watch our webinar on Curriculum Integration with Body Interact and learn how to transform your digital activities into meaningful clinical education.
References
Brauer, D. G., & Ferguson, K. J. (2015). The integrated curriculum in medical education: AMEE Guide No. 96. Medical Teacher, 37(4), 312–322. https://doi.org/10.3109/0142159X.2014.970998
Brown, K. M., Swoboda, S. M., Gilbert, G. E., Horvath, C., & Sullivan, N. (2023). Curricular integration of virtual reality in nursing education. Journal of Nursing Education, 62(6), 364–373. https://doi.org/10.3928/01484834-20230110-01
Dahri, K., MacNeil, K., Chan, F., Lamoureux, E., Bakker, M., Seto, K., & Yeung, J. (2019). Curriculum integration of virtual patients. Currents in Pharmacy Teaching and Learning, 11(12), 1309–1315. https://doi.org/10.1016/j.cptl.2019.09.007
Fąferek, J., Cariou, P. L., Hege, I., Mayer, A., Morin, L., Rodriguez-Molina, D., Sousa-Pinto, B., & Kononowicz, A. A. (2024). Integrating virtual patients into undergraduate health professions curricula: A framework synthesis of stakeholders’ opinions based on a systematic literature review. BMC Medical Education, 24(1), 727. https://doi.org/10.1186/s12909-024-05719-1
Reddi, S., & Javidi, D. (2025). A critical narrative review of medical school curricula: Teaching methods, assessment strategies, and technological integration. Cureus, 17(4), e82015. https://doi.org/10.7759/cureus.82015






