Body Interact advanced ventilatory algorithm with integrated blood gas physiology
When Ventilation Becomes Clinical Intelligence
Mechanical ventilation is one of the most critical interventions in intensive care medicine. (Hotz, Chang, Khemani, and Newth, 2026) Yet, too often, it is taught as a sequence of technical settings rather than as a structured clinical reasoning process.
By understanding the benefits and limitations of different ventilation modes and the goals of gas exchange, clinicians can choose a strategy that provides appropriate support while minimizing harm. The ventilator can also provide crucial diagnostic information in the form of respiratory mechanics. These, and the mechanical ventilation strategy, should be regularly reassessed (Szafran and Patel, 2024).
At Body Interact, the advanced ventilatory algorithm with integrated blood gas physiology takes this principle further. It transforms ventilator management from a sequence of settings into a structured process of clinical reasoning, linking ventilatory choices directly to patient physiology.
At Body Interact, we asked a fundamental question:
What if ventilation education did not start with settings, but with physiology?
What if every ventilatory adjustment were anchored in a structured understanding of gas exchange, acid–base balance, and compensatory mechanisms?
The result is the Advanced Ventilatory Algorithm with Integrated Blood Gas Physiology, a decision-making framework that transforms ventilation from a technical procedure into a clinical reasoning process.
Beyond Settings: Teaching the Logic Behind the Machine
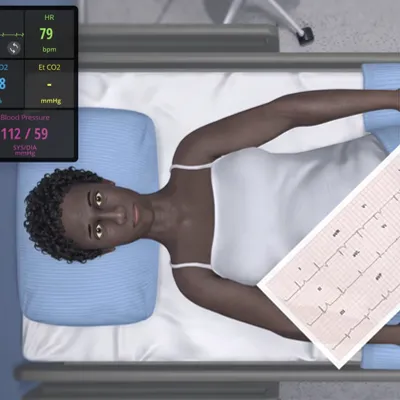
Every ventilator adjustment has consequences beyond a single parameter and directly influences oxygenation, carbon dioxide elimination, lung mechanics, and hemodynamics.
When PaCO₂ rises, it is not simply a value outside the normal range. It reflects an imbalance between CO₂ production and elimination. When pH drops, it signals a shift in homeostasis. When oxygenation worsens despite increasing FiO₂, the problem may not be oxygen delivery, but ventilation, perfusion mismatch, shunt, or compliance changes.
Traditional teaching often separates these domains. Students learn blood gas interpretation in one context and ventilator management in another. The connection between them is assumed rather than explicitly constructed. The Advanced Ventilatory Algorithm bridges this divide, requiring interpretation before intervention. By structuring this cognitive pathway, the algorithm ensures that adjustments are not reactive responses to abnormal values, but reasoned interventions aligned with the underlying pathophysiology.
Educational Impact: Making Reasoning Visible
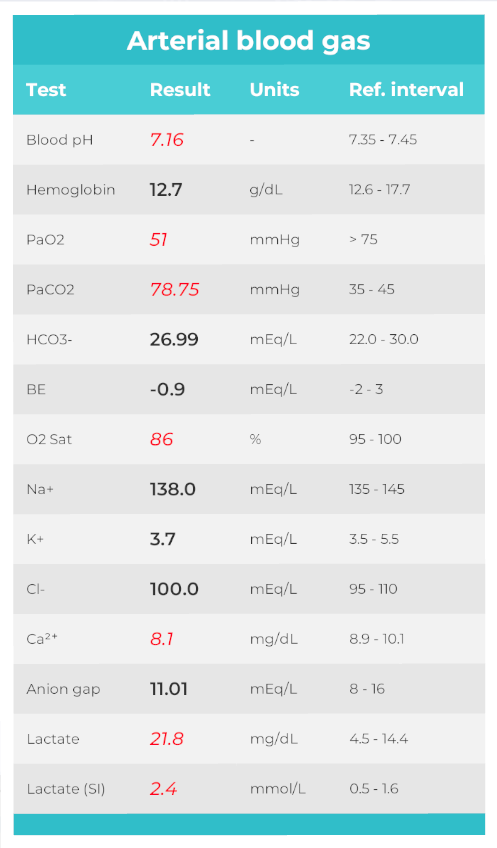
In clinical practice, arterial blood gases tell a story, and their analysis is a fundamental diagnostic tool in clinical medicine, offering critical insights into a patient’s respiratory and metabolic status (Mousavinejad et al 2026). They reflect compensation, progression, and sometimes impending failure. But that story only becomes meaningful when interpreted in context.
Within the algorithm, blood gas interpretation is not an isolated analytical exercise. It becomes the core of the decision-making process. Learners are guided to identify the primary disorder, evaluate compensatory mechanisms, and anticipate how ventilatory changes will influence the next physiological state.
For educators, one of the persistent challenges in teaching ventilation is assessing reasoning, not just correctness. A learner may select the appropriate setting, but for the wrong reason. Without visibility into their thought process, it is difficult to evaluate true competence.
The Advanced Ventilatory Algorithm makes reasoning explicit. It structures the cognitive path that leads to each intervention. In doing so, it supports competency-based education models, where understanding is valued over memorization.
It also allows learners to experience the consequences of suboptimal decisions in a safe environment. When physiology deteriorates in response to a miscalculated adjustment, the lesson becomes experiential rather than theoretical.
That experiential dimension is essential. Ventilation is not mastered through passive learning. It requires interaction with dynamic systems.
And when learners begin to think in systems rather than isolated values, something changes. That is the difference between operating a machine and managing respiratory failure.
And that difference is where education truly evolves.
Book a demo and discover how Body Interact can elevate mechanical ventilation training in your institution.
References
Szafran JC, Patel BK. Invasive Mechanical Ventilation. Crit Care Clin. 2024 Apr;40(2):255-273. doi: 10.1016/j.ccc.2024.01.003. Epub 2024 Feb 9. PMID: 38432695; PMCID: PMC12590542.
Hotz JC, Chang D, Khemani RG, Newth CJL. Decision Assist During Mechanical Ventilation. Respir Care. 2026 Feb;71(2):226-236. doi: 10.1177/19433654251384240. .
Mousavinejad SN, Lachouri R, Bahadorzadeh M, Khatami SH. Artificial intelligence for arterial blood gas interpretation. Clin Chim Acta. 2026 Jan 15;579:120691. doi: 10.1016/j.cca.2025.120691.
By Ana Santa – MSN, APRN
Editorial Manager